

INTRODUCTION
거대세포바이러스(cytomegalovirus, 이하 CMV) 감염은 고형장기 이식 후 가장 일반적이고 심각한 합병증 중 하나이다[1]. 우리나라에서는 CMV 항체 양성률이 3세에 80%, 6세에 90%, 9세 이상에서는 약 95 - 98%로 매우 높으나, 신장 이식 후에는 CMV 관련 질병이 약 5 - 13% [2,3], 간 이식 후에는 14%에서 발생한다[4]. 특히 장기이식 후나 림프성 종양과 관련된 경우 및 후천성 면역결핍 상태 등 T림프구-매개성 면역기능이 저하되는 경우 CMV 재활성 증후군이 발현되는 경우가 많다[5].
현재 임상에서는 CMV 감염 예방을 위해 두 가지 치료 전략이 주로 사용된다. 하나는 항바이러스제를 사용한 예방적 치료이고, 또 다른 하나는 정기적인 검사를 통해 CMV 복제(replication)가 확인된 환자를 위한 선제적 치료가 있다. 예방적 치료는 통상 이식 직후부터 3 - 6개월 간 지속하지만 이식 후 CMV 감염을 아예 없애지는 못하며, 과잉진료로 인한 항CMV 약물에 대한 내성 강화, 높은 약물치료 비용, 부작용 위험성 증가 등의 단점을 내포하고 있어 적절한 검사를 통한 치료방침 설정이 필요하다[1].
CMV-특이적 T 세포 면역 모니터링은 이식 전 및 이식 후 CMV 감염, CMV질환의 위험을 예측하여 적절한 치료방침을 결정할 수 있어[6,7], 다양한 분석법이 있으며, IL-2, TNF-α, CD107, programmed death-1 (PD-1), CD154 외에도 인터페론-감마(IFN-γ)가 유용한 바이오 마커로 사용되고 있다[8,9]. 검사방법으로는 CMV에 반응하여 인터페론 감마를 생성하는 T세포를 정량화하는 효소결합면역흡착점적법(enzyme-linked immunosorbent spot, ELISPOT), 인터페론 감마의 농도를 측정하는 효소결합면역흡착측정법(enzyme-linked immunosorbent assay, ELISA)이 있다.
이에 본 연구에서는 예측검사로서 거대세포바이러스 특이항원 자극 인터페론-감마 효소결합면역흡착점적법/ 효소결합면역흡착측정법의 안전성 및 유효성을 체계적 문헌고찰을 이용하여 평가하였다.
MATERIALS AND METHODS
1. 연구 설계
본 연구는 거대세포바이러스 특이항원 자극 인터페론-감마 효소결합면역흡착점적법/ 효소결합면역흡착측정법의 안전성 및 유효성을 체계적 문헌고찰 방법을 통하여 확인하였다. 핵심질문은 예측 검사의 목적에 맞춰 PICO (patient-index test-comparator-outcome)을 통해 작성하고 이를 바탕으로 검색어를 선정하여 문헌검색 및 최종 문헌선택 과정을 수행하였다.
2. 문헌 검색
1) PICO
본 연구의 관련 문헌 검토 후 임상전문가와의 논의를 통해 핵심질문을 확정하였다. 대상 환자(patients)는 고형장기 이식(예정) 환자, 조혈모세포 이식(예정) 환자, 면역억제요법 환자, 항암ㆍ방사선 치료 중인 종양 환자를 포함한 면역저하 환자로 하였으며 중재검사(index test)는 거대세포바이러스 특이항원 자극 인터페론-감마 효소결합면역흡착점적법, 거대세포바이러스 특이항원 자극 인터페론-감마 효소결합면역흡착측정법으로 하였다. 참고표준검사(reference test)는 배양검사, 혈청학적 검사, CMV 항체검사, CMV 항원혈증 검사, 중합효소연쇄반응법으로 보았으며, 의료결과(outcome)는 CMV 감염, 바이러스혈증, 재활성, 복제(replication), CMV 질환 등의 예후 관련 결과 발생의 예측도를 예후 관련 결과 발생의 위험, 카플란-마이어 생존 분석, 예후 관련 결과 발생에 대한 예측 정확성으로 평가하였다.
2) 문헌 검색 및 최종 문헌선택 과정
문헌 검색은 국내와 국외 데이터베이스로 나누어 2019년 10월 24일에 검색을 수행하였다. 국내 데이터베이스는 KoreaMed, 국립중앙도서관, 국회도서관, 국가자료공동목록시스템, 한국교육학술정보원, 학술데이터베이스검색, 과학기술학회마을, 한국의학논문데이터베이스를 이용하였고, 국외 데이터베이스는 MEDLINE, EMBASE, Cochrane Library를 이용하였다. 검색어는 각 데이터베이스별 특성을 고려하여 대상환자 및 중재시술에 초점을 맞추어 검색하였으며, 검색과정에서 언어는 제한하지 않았다. 검색전략에 따라 organ transplantation, solid organ transplant, solid organ transplant, immuno suppress, immuno inhibition, cytomegalovirus, CMV, interferon gamma, IFNgamma, enzyme-linked immunosorbent assay, enzyme-linked immunospot 등과 관련 검색어 활용 및 수기 검색을 포함하여 총 908편이 검색되었고, 중복 검색된 문헌 264편을 제외하였다.
문헌 선택 및 배제 기준은 PICO를 기반으로 선정하였고, 2명의 평가자는 다음의 기준에 따라 독립적으로 문헌을 선택하였다.
선택 기준은 면역저하 환자를 대상으로 한 연구, 거대세포바이러스 특이항원 자극 인터페론-감마 효소결합면역흡착점적법, 거대세포바이러스 특이항원 자극 인터페론-감마 효소결합면역흡착측정법을 수행한 연구이었고, 배제기준은 동물실험 또는 전임상시험 연구, 원저가 아닌 연구, 한국어 및 영어로 출판되지 않은 연구, 회색문헌, 중복 출판된 연구, 의료결과가 하나 이상 보고되지 않은 연구 등이었다.
1차적으로 초록을 중심으로 문헌을 선택하였고, 평가자간 문헌선택에 이견이 있는 경우 전문을 확인하거나 전문가 자문을 통해 최종적으로 총 25편의 임상시험연구를 선택하였다(Fig. 1).
3. 문헌의 질 평가
선택된 문헌의 질 평가는 영국 Scottish intercollegiate guidelines network (SIGN)의 방법론 체크리스트를 이용하였으며[10], 2명의 평가자가 독립적으로 수행하였다. 질 평가 결과, 평가자간 이견이 있는 부분은 논의를 통해 해결하였다.
SIGN의 질 평가 도구는 연구유형에 따라 필수항목을 선정하고, 질 평가항목에 거의 모든 또는 모든 기준이 충족되는 경우 ‘++’, 몇 가지 기준이 충족된 경우 ‘+’, 거의 모든 또는 모든 기준이 충족되지 않는 경우 ‘-’ 로 평가하였으며, 평가자간 질 평가 결과에 이견은 없었으며, 관련 문헌의 질 평가 결과는 모두 ‘2+’ 이었다. 근거수준도 SIGN 도구를 이용하여 질 평가 결과에 따른 근거수준을 판정하였다[10].
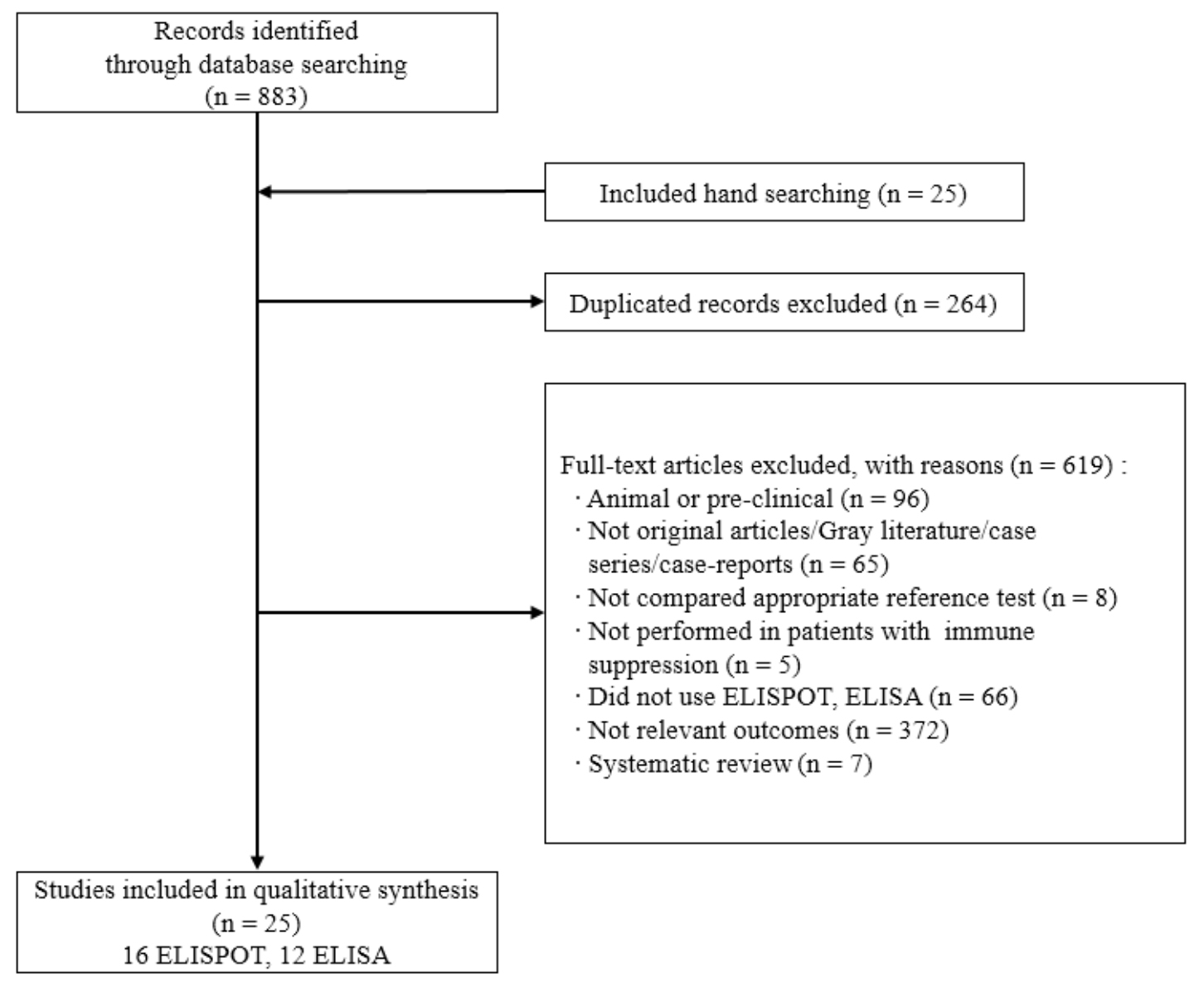
Fig. 1. Flow chart of literature selection process.
ELISPOT, enzyme-linked immunospot; ELISA, enzyme-linked immunosorbent assay.
4. 자료 추출
자료 추출은 시범적 검토를 거친 후, 임상 전문가의 의견을 반영하여 서식을 확정하였다. 문헌에 기술된 일반적인 정보와 각 문헌별로 결과에 영향을 주는 연구 특성 및 결과측정 등 안전성 및 유효성에 대한 자료를 추출하였다. 정확한 추출을 위하여 여러 차례 반복하여 수행한 뒤 진단검사의학과, 신장내과, 혈액종양내과, 감염내과, 외과, 소아청소년과 전문가 총 8인으로 구성된 임상전문가 회의를 통해 최종 확인하였다.
5. 자료 분석
자료 분석은 정성적 분석 방법을 적용하여 시행하였으며, 각 연구별 정량적 분석이 가능한 의료결과가 부족하여 정량적 분석은 수행하지 않았다. 동 기술의 안전성 및 유효성은 검사방법별, 검사목적별로 기술하였다.
RESULTS
1. 대상 문헌의 일반 특성
본 연구에 선택된 문헌은 총 25편으로 효소결합면역흡착점적법은 16편이었고[6,7,11-24], 효소결합면역흡착측정법은 12편이었으며[1,12,16,24-32], 3편[12,16,24]에서는 이 두 검사법에 대한 결과를 함께 제시하고 있었다. 이식환자별로는 신장이식 환자 13편[1,6,12-20,22], 고형장기이식 환자 3편[25,28,32], 간이식 환자 5편[23,26,27,30,31], 조혈모세포이식 환자 3편[21,24,29], 혈액투석 환자 1편[11]으로 84% (21/25편)가 고형장기이식 환자이었다. 인종은 주요 3개 인종인 아시아인, 흑인, 백인으로 구분하였고, 아시아인 5편[7,16,17,23 24]을 제외한 연구는 모두 백인이었다(Table 1).
2. 동 기술의 안전성
동 기술의 안전성은 환자의 혈액을 채취하여 체외에서 이루어지므로 환자에게 직접적인 위해를 가하지 않아 검사수행에 따른 안전성에는 문제가 없는 것으로 평가하였다.
3. 동 기술의 유효성
동 기술의 유효성은 예후 관련 결과 발생의 위험도, 카플란–마이어 생존분석(표에 제시하지 않음), 예후 관련 결과 발생에 대한 예측 정확성을 통해 평가하였다. 예후 관련 결과는 CMV 감염, 재활성, 복제, CMV 질환 등의 CMV 사건발생으로 보았다. 평가 결과는 검사방법별, 검사목적별(이식 후 예후 〮 예측, 예방적/선제적 치료 후 치료방침 결정)로 구분하여 제시하였다.
1) 효소결합면역흡착점적법(enzyme-linked immunosorbent spot, ELISPOT)
효소결합면역흡착점적법의 예후 관련 결과 발생 위험도는 16편의 연구에서 보고되었다[6,7,12-24]. 추적 관찰 기간은 1 - 55개월까지이었고, CMV 세포면역반응에 대한 임계치는 언급되지 않거나, 20SFU/2×105, 3×105 PBMCs, spot수가 2, 3배 증가한 경우 등 다양하게 보고되었다(Table 1).
첫째, 이식 후 예후 〮 예측은 13편의 연구에서 보고되었다[6,7,11,13,16-24]. CMV 사건발생 위험비(Hazard Ratio)를 보고한 2편[22,23]과 CMV 사건발생 오즈비(Odds ratio)를 보고한 2편[18,20]에서 검사결과 활성군 대비 비활성 군에서 CMV 사건발생 오즈비가 유의하게 높게 보고되었다. 카플란 마이어 곡선은 5편에서 검사결과 활성군 대비 비활성 군에서 CMV 사건 발생률이 높았으나[6,13,17,21,23], 1편에서만 통계적으로 유의하지 않았다[6]. 예측 진단정확성을 확인한 연구는 12편이었고[6,7,11,13,16,17-19,21-24], 민감도 0.08 - 1.00, 특이도 0.14 - 1.00, 양성예측도 0.21 - 1.00, 음성예측도 0.48 - 1.00, 검사정확도 0.36 - 0.92, AUC 0.69 - 0.85이었다(Table 2).
둘째, 예방적/선제적 치료 후 치료방침 결정은 3편의 연구에서 보고되었다[12,14,15]. 이식 후 예방적 치료를 받은 신장이식 환자에서 12개월 시점에서 CMV 사건발생 오즈비는 활성군 대비 비활성 군에서 유의하게 높게 보고되었다. 카플란 마이어 곡선은 2편[14,15]에서 검사결과 활성군 대비 비활성 군에서 CMV 사건 발생률이 유의하게 높았다. 예방적 치료 후 치료방침 결정을 위한 예측 진단정확성은 3편이었고[12,14,15], 민감도 0.57 - 0.83, 특이도 0.65 - 0.80, 양성예측도 0.91 - 0.98, 음성예측도 0.15 - 0.90이었고, AUC는 0.63 - 0.76이었다(Table 2).
2) 효소결합면역흡착측정법(enzyme linked immunosorbent assay, ELISA)
효소결합면역흡착측정법의 예후 관련 결과 발생 위험도는 12편의 연구에서 보고되었다[1,11,16,24-32]. 추적 관찰 기간은 6 - 24개월까지이었고, CMV 세포면역반응에 대한 임계치는 0.1 또는 0.2 IU/mL이었다(Table 3).
첫째, 이식 후 예후 〮 예측은 8편의 연구에서 보고되었다[11,16,24-27,29,30]. 예후 관련 결과 발생의 위험도는 각각 1편에서 검사결과 활성군 대비 비활성군에서 CMV 사건발생 위험비 또는 CMV 사건발생 오즈비가 유의하게 높게 보고되었고[25,30], 카플란-마이어 생존 분석은 활성군 대비 비활성군에서 사건 발생률이 높았으나 통계적으로 유의하지 않았다[30]. 예후 관련 결과 발생에 대한 예측 정확성(8편)은 민감도 0.14 - 0.86, 특이도 0.53 - 1.00, 양성예측도 0.29 - 0.93, 음성예측도 0.24 - 0.85로 모두 범위가 넓었다[11,16, 24, 26-30] (Table 3).
둘째, 예방적/선제적 치료 후 치료방침 결정은 4편에서 보고되었다[1,28,31,32]. 예후 관련 결과 발생의 위험도는 1편에서 검사결과 활성군 대비 비활성군에서 위험비가 유의하게 높게 보고되었고[1], 카플란-마이어 생존 분석도 4편에서 모두 검사결과 활성군 대비 비활성군에서 사건 발생률이 유의하게 높았으나[1,29,32,33], 1편에서만 통계적으로 유의하지 않았다[32]. 예후 관련 결과 발생에 대한 예측 정확성은[28,31] 민감도 1.00, 0.30, 특이도 0.89, 0.93, 양성예측도 0.33, 0.93, 음성예측도 1.00, 0.27이었다(Table 3).
DISCUSSION
거대세포바이러스 특이항원 자극 인터페론-감마 효소결합면역흡착점적법/ 효소결합면역흡착측정법은 고형장기이식환자를 포함한 면역억제환자에서 CMV 감염을 예측하여 적절한 치료 방침을 결정하기 위한 면역모니터링 검사의 필요성이 대두되고 있다.
The Transplantation Society 가이드라인에서는 CMV 특이적 세포 면역 모니터링이 다수의 연구에서 고형장기 이식 전 및 이식 후 환경에서 CMV 감염을 예측하고, 모니터링을 통해 CMV 질환의 위험을 층화하여, 선제적/예방적 치료시 약제 중단/사용여부를 결정하고, 약제 중단 후 CMV 질환 재발에 대하여 철저한 감시여부를 확인할 수 있는 검사로 권고하고 있었고, 향후 임계치 등 검사의 표준화에 대한 추가 연구가 필요하다고 제시하고 있었다[9,33]. The American Society of Transplantation (2019)에서는 고형장기이식 후의 면역학적 모니터링은 CMV 질환의 위험을 층화하기 위해 사용될 수 있지만, 특정 림프구 임계치는 임상적으로 검증되어야한다고 제시하였다(weak, low)[34].
동 기술과 관련된 체계적 문헌고찰은 Ruan 등(2019)의 연구가 확인되었다. 신장이식 환자를 대상으로만 동 검사가 CMV DNA 혈증과 CMV 감염의 면역모니터링으로서 진단정확성을 분석하였다. 메타분석 결과, ELISPOT (10편)의 통합민감도는 0.73 (95% CI, 0.67 - 0.78), 통합특이도는 0.61 (95 % CI, 0.56 - 0.65)이었고, ELISA (6편)는 통합민감도 0.38 (95 % CI, 0.28 - 0.49), 통합 특이도 0.38 (95 % CI, 0.32 - 0.44)으로 ELISPOT은 CMV 감염의 진단과 예측을 잘 수행하나, ELISA는 추가 연구가 필요하다고 결론내리고 있었다[35].
본 연구에서는 동 검사의 안전성 및 유효성을 평가하기 위하여 ELISPOT 16편[6,7,12-24], ELISA 12편[1,11,16,24-32]으로 총 25편의 연구(코호트 연구 15편, 진단법 평가연구 10편)를 선택하여 평가하였다. 임계치는 ELISA는 상용화된 검사시약의 임계치를 개발사에서 제시하고 있었으나, ELISPOT의 경우 검사실 검사로 연구들에서 다양하게 사용되고 있었다.
동 검사의 유효성은 선택된 연구의 76% (19/25편)가 고형장기 이식환자이었다. Manuel (2013)의 다기관 연구에서 고형장기 이식 후 예방적 치료 후 ELISA검사가 저위험군, 중간위험군, 고위험군으로 층화하여 CMV 질환을 예측가능하다는 결과를 제시하였다[28]. 다른 선택된 연구들에서도 이식 전 예후 예측, 예방적/선제적 치료 후 예후 예측(late onset CMV)에 대하여 예후 관련 결과 발생의 위험도, 카플란-마이어 생존분석 결과가 활성 대비 비활성인 경우 사건 발생률이 유의하게 높게 보고되고 있어 동 검사가 진료방침을 결정할 수 있는 검사로 가치가 있었으나, 임계치가 다양하였고, 예측 정확도의 범위가 넓게 보고되었다. 또한, 조혈모세포이식 환자를 대상으로 한 연구는 3편이 확인되었으나, 조혈모세포이식 환자는 T림프구의 측정, CMV에 대한 예방적 항바이러스제 약제 사용이 필요하지 않아 동 검사의 유용성이 낮았다.
결론적으로, 거대세포바이러스 특이항원 자극 인터페론-감마 효소결합면역흡착점적법/ 효소결합면역흡착측정법은 CMV 질환의 위험을 층화하여 고형장기 이식환자의 예방적/선제적 치료의 방침을 결정할 수 있는 잠재성이 있는 검사이나, 임계치 확립과 검사의 표준화를 위하여 추가적인 문헌적 근거가 필요하다.
요약
배경: 거대세포바이러스 특이항원 자극 인터페론-감마 효소결합면역흡착점적법/효소결합면역 흡착측정법은 면역저하환자에서 CMV 감염/질환의 위험 예측검사로서 안전성 및 유효성을 체계적 문헌고찰 방법을 통하여 확인하고자 하였다.
방법: 문헌 검색은 MEDLINE, EMBASE 및 Cochrane library를 포함한 전자 데이터베이스를 통해 수행되었으며, 884편이 검색되었다. 최종적으로 선택된 문헌은 25편(코호트 연구 15편, 단면 연구 10편)으로 연구대상이 고형장기 이식환자, 조혈모세포 이식환자, 혈액투석 환자이었다. 두 명의 연구자는 독립적으로 자료 추출 및 문헌의 질평가를 수행하였다.
결과: 선택된 대부분의 연구는 고형장기 이식환자를 대상으로 한 연구였다. 동 검사는 체외에서 이루어지는 검사로 안전하다. 유효성은 대부분이 예후 관련 결과 발생의 위험도는 검사결과 활성군 대비 비활성군에서 CMV 사건발생(CMV 감염, CMV 질환 등) 위험비 또는 오즈비가 유의하게 높았고, 카플란-마이어 생존분석 결과에서도 CMV 사건 발생률이 유의하게 높았다. 그러나, CMV 세포면역반응에 대한 임계치가 다양하였고, 예측 정확도의 범위가 넓게 보고되었다.
결론: 거대세포바이러스 특이항원 자극 인터페론 감마 효소결합면역흡착점적법/효소결합면역흡착측정법은 고형장기 이식환자에서는 CMV 감염/질환의 위험을 층화하여 예방적/선제적 치료의 방침을 결정할 수 있는 잠재성이 있는 검사이나, 임계치 확립과 검사의 표준화를 위하여 추가적인 문헌적 근거가 필요하다.

