Young Bok Lee![]() , Mingyu Kim
, Mingyu Kim , Dong Soo Yu
, Dong Soo Yu

1. Segal E and Elad D. Human and zoonotic dermatophytoses: epidemiological aspects. Front Microbiol 2021;12:713532.


2. Chanyachailert P, Leeyaphan C, Bunyaratavej S. Cutaneous fungal infections caused by dermatophytes and non-dermatophytes: an updated comprehensive review of epidemiology, clinical presentations, and diagnostic testing. J Fungi 2023;9:669.
3. Zacharopoulou A, Tsiogka A, Tsimpidakis A, Lamia A, Koumaki D, Gregoriou S. Tinea incognito: challenges in diagnosis and management. J Clin Med 2024;13:3267.
4. Havlickova B, Czaika VA, Friedrich M. Epidemiological trends in skin mycoses worldwide. Mycoses 2008;51(Suppl 4):2-15.
5. Ali-Shtayeh MS, Yaish S, Jamous RM, Arda H, Husein EI. Updating the epidemiology of dermatophyte infections in Palestine with special reference to concomitant dermatophytosis. J Mycol Med 2015;25:116-22.
6. Foster KW, Ghannoum MA, Elewski BE. Epidemiologic surveillance of cutaneous fungal infection in the United States from 1999 to 2002. J Am Acad Dermatol 2004;50:748-52.
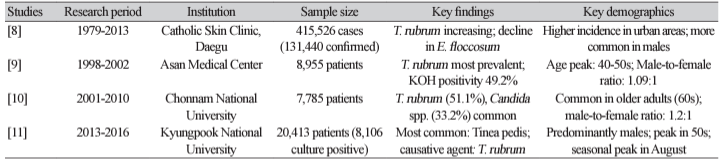
7. Lee WJ, Kim SL, Jang YH, Lee SJ, Kim DW, Bang YJ, et al. Increasing prevalence of Trichophyton rubrum identified through an analysis of 115,846 cases over the last 37 years. J Korean Med Sci 2015;30:639-43.
8. Kim SL, Lee KC, Jang YH, Lee SJ, Kim DW, Lee WJ, et al. The epidemiology of dermatophyte infection in Southeastern Korea (1979~2013). Ann Dermatol 2016;28:524-7.
9. Lee DK, Moon KC, Koh JK. Clinical and mycological studies on superficial fungal infection. Korean J Med Mycol 2006;11:54-63.
10. Lee YW, Yoon SJ, Lee JB, Kim SJ, Lee SC, Won YH. Clinical and mycological studies on dermatomycosis (2001-2010). Korean J Med Mycol 2013;18:30-8.
11. Lee WJ, Eun DH, Jang YH, Bang YJ, Jun JB. The incidences of dermatophytosis and cutaneous candidiasis infection in Southeastern Korea between 2013 and 2016. Korean J Med Mycol 2018;23:1-8.
12. Jang SJ and Ahn KJ. Superficial dermatomycosis and the causative agents in Korea. Korean J Med Mycol 2004;9:91-9.
13. Ward H, Parkes N, Smith C, Kluzek S, Pearson R. Consensus for the treatment of tinea pedis: a systematic review of randomised controlled trials. J Fungi 2022;8:351.
14. Cho M, Lee YW, Lee DH, Jeong KH, Kwon SH, Kim JE, et al. A survey on the perception and behavior regarding tinea pedis among Korean adults. Korean J Dermatol 2023;61:420-8.
15. Lee SK, Choi JS, Kim KH. A Clinical and mycological study of tinea pedis. Korean J Dermatol 1995;33:1029-37.
16. Seo KI, Kim JA, Lim JG, Eun HC, Youn JI. Prevalence of tinea pedis in Korean soldiers in a battalion. Korean J Dermatol 2000;38:1050-4.
17. Taplin D. Superficial mycoses. J Invest Dermatol 1976;67:177-81.
18. Aly R. Ecology and epidemiology of dermatophyte infections. J Am Acad Dermatol 1994;31:S21-5.
19. Park SH, Shin YM, Moon SK, Shin DH, Choi JS, Kim KH, et al. A clinical and mycological study of tinea pedis. Korean J Med Mycol 2006;11:123-31.
20. Jang SJ, Choe YB, Ahn KJ. A clinical and mycological study of tinea corporis. Korean J Dermatol 2004;42:166-72.
21. Higgins EM, Fuller LC, Smith CH. Guidelines for the management of tinea capitis. Br J Dermatol 2000;143:53-8.
22. Gianni C, Betti R, Perotta E, Crosti C. Tinea capitis in adults. Mycoses 1995;38:329-31.
23. He M, Zeng J, Mao Y, Zheng Y, Lian X, Chen H. Aetiological changes of tinea capitis in the Hubei area in 60 years: focus on adult tinea capitis. Mycoses 2021;64:1527-34.
24. Khosravi AR, Shokri H, Vahedi G. Factors in etiology and predisposition of adult tinea capitis and review of published literature. Mycopathologia 2016;181:371-8.
25. Liang G, Zheng X, Song G, Zhang M, Liu J, Zang X, et al. Adult tinea capitis in China: a retrospective analysis from 2000 to 2019. Mycoses 2020;63:876-88.
26. Park SK, Park SW, Yun SK, Kim HU, Park J. Tinea capitis in adults: a 18-year retrospective, single-centre study in Korea. Mycoses 2019;62:609-16.
27. Lee HJ, Kim JY, Park KD, Jang YH, Lee SJ, Bang YJ, et al. Analysis of adult patients with tinea capitis in Southeastern Korea. Ann Dermatol 2020;32:109-14.
28. Lee YW, Lim SH, Yim SM, Choe YB, Ahn KJ. A clinical and mycological study of dermatophytosis associated with animal contact. Korean J Med Mycol 2005;10:151-9.
29. Seong M, Son H, Suh MK, Lee K. Clinical and mycological analysis of tinea capitis in adults and children during the last 24-year-period (1999~2022): a single-center study. Korean J Dermatol 2024;62:82-91.
30. Jung IS, Ryu GW, Yun SJ, Lee JB, Kim SJ, Lee SC, et al. Clinical and mycological features of tinea capitis in Korea: analysis of 61 cases from 1990 to 2018. Korean J Dermatol 2020;58:16.
31. Rodriguez-Pazos L, Pereiro-Ferreirós MM, Pereiro M Jr, Toribio J. Onychomycosis observed in children over a 20-year period. Mycoses 2011;54:450-3.
32. Lange M, Roszkiewicz J, Szczerkowska-Dobosz A, Jasiel-Walikowska E, Bykowska B. Onychomycosis is no longer a rare finding in children. Mycoses 2006;49:55-9.
33. Ghannoum MA, Hajjeh RA, Scher R, Konnikov N, Gupta AK, Summerbell R, et al. A large-scale North American study of fungal isolates from nails: the frequency of onychomycosis, fungal distribution, and antifungal susceptibility patterns. J Am Acad Dermatol 2000;43:641-8.
34. Gupta AK, Jain HC, Lynde CW, Macdonald P, Cooper EA, Summerbell RC. Prevalence and epidemiology of onychomycosis in patients visiting physicians’ offices: a multicenter Canadian survey of 15,000 patients. J Am Acad Dermatol 2000;43:244-8.
35. Zaias N. Onychomycosis. Arch Dermatol 1972;105:263-74.
36. Baran R and Hay RJ. New clinical classification for onychomycoses. J Mycol Med 2014;24:247-60.
37. Lim SW, Suh MK, Ha GY. Clinical features and identification of etiologic agents in onychomycosis (1999-2002). Korean J Dermatol 2004;42:53-60.
38. Kim NH, Yun SJ, Lee JB, Kim SJ, Lee SC, Won YH. Clinical study of onychomycosis observed in children (2005~2014). Korean J Dermatol 2016;54:781-7.
39. Drake LA, Dinehart SM, Farmer ER, Goltz RW, Graham GF, Hardinsky MK, et al. Guidelines of care for superficial mycotic infections of the skin: tinea corporis, tinea cruris, tinea faciei, tinea manuum, and tinea pedis. J Am Acad Dermatol 1996;34:282-6.
40. Yim SM, Choi YB, Ahn KJ. A clinical and mycological study of tinea faciale. Korean J Med Mycol 2004;9:214-21.
41. Noguchi H, Jinnin M, Miyata K, Hiruma M, Ihn H. Clinical features of 80 cases of tinea faciei treated at a rural clinic in Japan. Drug Discov Ther 2014;8:245-8.
42. Hur W, Koo SW, Hann SK, Bang D. Two cases of tinea faciei with atypical clinical manifestation. Korean J Dermatol 1991;29:414-8.
43. Park SB, Lee YW, Park EJ, Kwon IH, Kim KH, Kim KJ. A case of tinea faciei caused by Trichophyton mentagrophytes with atypical presentation. Korean J Med Mycol 2010;15:170-4.
44. Hwang J, Kang JM, Ahn JG. Two cases of tinea faciei mimicking eczema herpeticum in siblings. Pediatr Infect Vaccine 2021;28:49-56.
45. Kim WJ, Park JW, Shin DH, Choi JS, Kim KH. Three cases of tinea faciei misdiagnosed as contact dermatitis. Korean J Med Mycol 2004;9:54-9.
46. Kang GS, Hwang SM, Suh MK, Ha GY, Jang TJ. A case of rosacea-like tinea faciei caused by Trichophyton rubrum. Korean J Med Mycol 2010;15:22-6.
47. Kim I, Bang YJ, Jun JB, Park KD, Chung H, Park J. The clinical and mycological study of tinea faciei in Daegu. Korean J Med Mycol 2015;20:63-9.
48. Shin DH and Kim KH. Clinical and mycologic studies of tinea cruris. Korean J Dermatol 1999;37:219-24.
49. Lim JW, Suh MK, Ha GY. The frequency of tinea pedis in patients with tinea cruris. Korean J Med Mycol 2007;12:1-8.
50. Daniel CR 3rd, Gupta AK, Daniel MP, Daniel CM. Two feet-one hand syndrome: a retrospective multicenter survey. Int J Dermatol 1997;36:658-60.
51. Mochizuki T, Takeda K, Nakagawa M, Kawasaki M, Tanabe H, Ishizaki H. The first isolation in Japan of Trichophyton mentagrophytes var. erinacei causing tinea manuum. Int J Dermatol 2005;44:765-8.
52. Rhee DY, Kim MS, Chang SE, Lee MW, Choi JH, Moon KC, et al. A case of tinea manuum caused by Trichophyton mentagrophytes var. erinacei: the first isolation in Korea. Mycoses 2009;52:287-90.
53. Lim JH, Kim HS, Kim HO, Cho BK, Kim SI, Choi JS, et al. Tinea manus caused by Trichophyton mentagrophytes var. erinacei transferred from a hedgehog. Korean J Dermatol 2009;47:504-7.
54. Lee S and Ahn HJ. Pustular tinea manuum in a child caused by Trichophyton erinacei from a pet hedgehog. Korean J Dermatol 2023;61:204-6.
55. Ko D, Kim I, Chae I, Park KD, Chung H, Bang YJ, et al. The clinical and mycological study of tinea manus and concomitant dermatophytosis. Korean J Med Mycol 2013;18:102-10.
56. Lee JH, Kang JW, Nam MW, Lee JS. Investigating the diagnostic utility of potassium hydroxide (KOH) smear test and the influence of clinical and practical factors in onychomycosis. Korean J Dermatol 2024;62:228-33.
57. Baek G, Koo T, Lee D, Kang HJ, Kim MS, Kim Y, et al. Histopathological examination of the nail plate and comparison between periodic acid-schiff and gomori’s methenamine silver stains for the diagnosis of onychomycosis. Korean J Dermatol 2021;59:618-23.
58. Jung MY, Shim JH, Lee JH, Lee JH, Yang JM, Lee DY, et al. Comparison of diagnostic methods for onychomycosis, and proposal of a diagnostic algorithm. Clin Exp Dermatol 2015;40:479-84.