The global prevalence of carbapenemase-producing Enterobacterales(CPE) has been increasing recently, posing a substantial threat to infection control [1,2]. In particular, the importance of environmental factors in CPE transmission has been recognized, and the potential for transmission through the environment has been demonstrated in outbreak cases [3]. Consequently, environmental management is important in CPE infection control.
Environmental culture involves collecting and culturing specimens from air, water, and environmental surfaces. When conducted properly, environmental culture can support epidemiological investigations and aid in determining the effectiveness of infection control measures; however, if conducted improperly, it can lead to wastage of clinical microbiology laboratory and infection control resources, and misleading data can lead to incorrect infection control measures. The purpose of environmental cultures is twofold: to monitor compliance with hygienic standards and detect the presence or absence of specific healthcare-associated infectious pathogens. The second is generally undertaken during outbreak investigations [4]. In cases involving carbapenem-resistant Enterobacterales (CRE), the Korean infection control guidelines recommend environmental culture testing in the event of an outbreak [5].
However, few studies have investigated environmental cultures for CPE in Korea [6,7]. In the present study, we conducted environmental cultures for CPE to evaluate the environmental contamination around patients with CPE.
Nine intensive care unit (ICU) inpatients with CPE isolated from clinical specimens referred for culture between March 2017 and October 2017 were included. Clinical information such as sex, age, ward, medical department, comorbidities, hospitalization history, and clinical microbiology results were collected by reviewing electronic records. The specimens were collected from bed railings/controls, headboards, intravenous poles, call buttons, telephones, bedside tables, chairs, sinks, light switches, door handles, bathroom door handles, bathroom light switches, bathroom-assisted handles, toilet handles, bathroom sinks, and toilet seats. Additionally, specimens were collected from infusion pumps, monitor controls, monitor control touch screens, monitor cables, and ventilator controls. Culture for CPE detection was performed by incubating 10 μg meropenem disks in trypticase soy broth overnight followed by overnight incubation in MacConkey agar in accordance with the Centers for Disease Control and Prevention laboratory guidelines [8]. Identification of isolates and antimicrobial susceptibility testing were performed using the VITEK2 system (bioMérieux, Durham, NC, USA). RAPIDEC CARBA NP (bioMérieux, Marcy-l’Étoile, France) and Xpert Carba-R (Cepheid, Sunnyvale, CA, USA) tests were conducted to detect and genotype the carbapenemases.
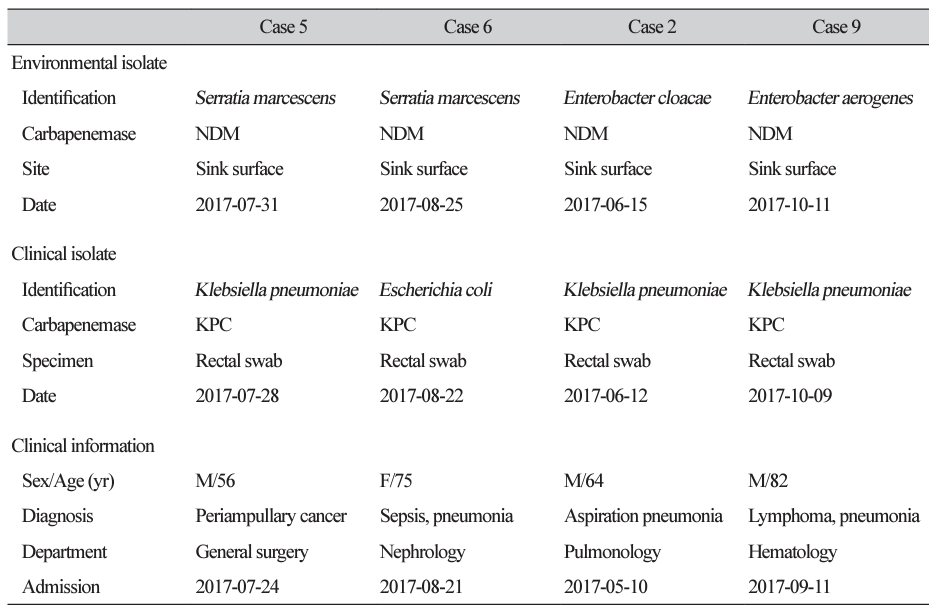
CPE was detected in the environmental cultures of four of the nine cases (Table 1). All four isolates were collected from sink surfaces in isolation rooms within the ICU (Fig. 1). Environmental isolates were identified as Serratia marcescens (n = 2), Enterobacter cloacae (n = 1), and Enterobacter aerogenes (n = 1). All four isolates harbored blaNDM. CPE isolates from the environment differed from those isolated from patients and had different carbapenemases. In all cases, Acinetobacter baumannii and Pseudomonas aeruginosa were detected at various environmental sites (data not shown). In Case 2, environmental cultures were conducted again after the source was disinfected, and CPE was not isolated.
Associations between water environments in hospitals and healthcare-associated infections have been reported [3,9]. Healthcare water environments, including potable water, faucets, sink surfaces, and wastewater drainage systems such as drains, sink/shower traps, toilets, and drainage pipes, can serve as reservoirs for nosocomial pathogens such as drug-resistant Enterobacterales, Pseudomonas spp., and A. baumannii [3]. This study found that sink surfaces were a major source of contamination by multidrug-resistant organisms, including CPE and P. aeruginosa. Similarly, previous reports have shown that sinks are a reservoir for CPE, are associated with CPE in patients, and are a transmission source [6,10,11].
Reports indicate that CPEs in the environment are associated with CPEs isolated from patients and may even cause outbreaks [6,12,13]. However, in this study, the carbapenemase genes of CPEs isolated from the environment differed from those of CPEs isolated from patients (the environmental isolates were all blaNDM, and the patient isolates were blaKPC), suggesting that the environmental and patient isolates were unrelated. Environmental cultures were performed in most cases shortly after isolation was initiated. Considering the timing of these procedures, environmental isolates were presumed to be present in the environment, regardless of the occurrence of CPE carriers.
This study has several limitations. The study included a small number of cases. In addition, the original study plan was to perform environmental cultures where the patient was staying when the CPE was isolated; however, this was possible only in one case. In other cases, the environmental culture was performed at the location where the patient was isolated after CPE isolation (isolation room in the ICU). This was due to the time required to identify the target cases, as it typically took more than 3 days to report CPE during the study period, and we were unable to delay patient isolation and disinfection for research purposes because of the priority of patient care and infection control. Further studies are needed to demonstrate the horizontal transmission of blaNDM among environmental isolates.
In the present study, we detected CPEs carrying blaNDM in sinks in the ICU, which were not associated with the isolation of CPEs from patients. However, the repeated isolation of CPE from sinks over several months is alarming. More aggressive disinfection and environmental surveillance are needed to prevent contamination by CPE and other multidrug-resistant organisms in ICUs.