1. Protano C, Cammalleri V, Romano Spica V, Valeriani F, Vitali M. Hospital environment as a reservoir for cross transmission: cleaning and disinfection procedures. Ann Ig 2019;31:436-48.

2. Han Z, Pappas E, Simmons A, Fox J, Donskey CJ, Deshpande A. Environmental cleaning and disinfection of hospital rooms: a nationwide survey. Am J Infect Control 2021;49:34-9.
3. Kampf G, Kramer A. Epidemiologic background of hand hygiene and evaluation of the most important agents for scrubs and rubs. Clin Microbiol Rev 2004;17:863-93. 
4. Martínez JA, Ruthazer R, Hansjosten K, Barefoot L, Snydman DR. Role of environmental contamination as a risk factor for acquisition of vancomycin-resistant enterococci in patients treated in a medical intensive care unit. Arch Intern Med 2003;163:1905-12.
5. Weber DJ, Rutala WA, Miller MB, Huslage K, Sickbert-Bennett E. Role of hospital surfaces in the transmission of emerging health care-associated pathogens: norovirus, Clostridium difficile, and Acinetobacter species. Am J Infect Control 2010;38:S25-33.
6. Center for Disease Control and Prevention. Best Practices for Environmental Cleaning in Healthcare Facilities: in Resource-limited Settings. https://www.cdc.gov/healthcare-associated-infections/media/pdfs/environmental-cleaning-rls-508.pdf [Online] (last visited on 23 August 2024).
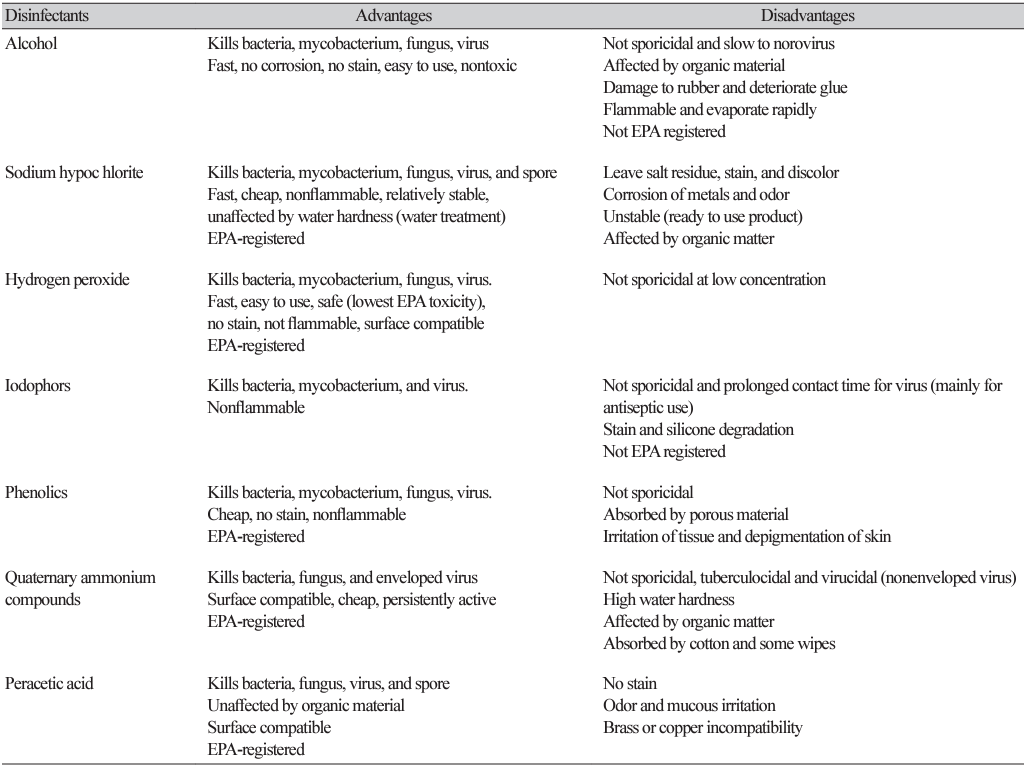
7. Rutala WA, Weber DJ. Disinfection and sterilization in health care facilities: an overview and current issues. Infect Dis Clin North Am 2021;35:575-607.
8. Fram DS, Medeiros EA, Ribeiro RM, Escudero DVDS, Alves JCD, Macedo B, et al. High-touch surfaces disinfection compliance in a COVID-19 intensive care unit. Am J Infect Control 2023;51:469-71.
9. Lakshminarayanan R, Ramakrishna S, Mondal DP, Srivastava AK, Dhand C. Recent advances in copper and copper-derived materials for antimicrobial resistance and infection control. Curr Opin Biomed Eng 2022;24:100408.
10. Querido MM, Aguiar L, Neves P, Pereira CC, Teixeira JP. Self-disinfecting surfaces and infection control. Colloids Surf B Biointerfaces 2019;178:8-21.
11. Tsou AY, Pavlides S, Koepfler L, Drummond C. No-touch modalities for disinfecting patient rooms in acute care settings: a rapid review. Rockville (MD): Agency for Healthcare Research and Quality (US); 2020 Oct 2. Report No.: 20(21)-EHC021.
12. Obenza A, Cruz P, Buttner M, Woodard D. Microbial contamination on ambulance surfaces: a systematic literature review. J Hosp Infect 2022;122:44-59.
13. Leas BF, Sullivan N, Han JH, Pegues DA, Kaczmarek JL, Umscheid CA. Environmental cleaning for the prevention of healthcare-associated infections. Rockville (MD): Agency for Healthcare Research and Quality (US); 2015 Aug. Report No.: 15-EHC020-EF.
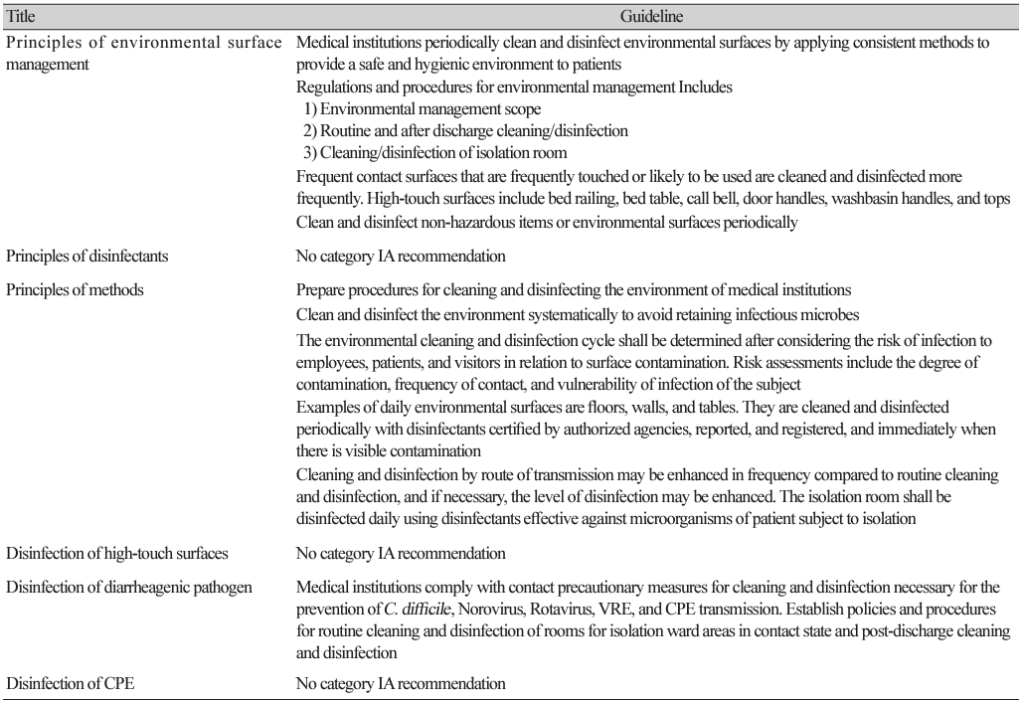
14. Infection Control Consulting Network. Recommendations for cleaning and disinfection of environmental surfaces in medical institutions. https://www.iccon.or.kr/rang_board/list.html?num=1614&start=30&code=iccons_guide [Online] (last visited on 23 August 2024).
15. Abubakar U, Al-Anazi M, Alanazi Z, Rodríguez-Baño J. Impact of COVID-19 pandemic on multidrug resistant gram positive and gram-negative pathogens: a systematic review. J Infect Public Health 2023;16:320-31.